
ADHD Combined Presentation Explained for Adults
ADHD combined presentation is defined as a pattern in which a person meets the full clinical symptom threshold for both inattention and hyperactivity-impulsivity at the same time. The formal term used in the DSM-5-TR is “ADHD, combined presentation,” and it is the most clinically recognized form of the condition in adults seeking evaluation. According to the U.S. CDC, ADHD is classified into three presentations: predominantly inattentive, predominantly hyperactive-impulsive, and combined. Understanding which presentation applies to you matters because it directly shapes how treatment is structured and what symptoms to prioritize. If you have been wondering what is ADHD combined presentation and whether it fits your experience, this guide gives you the clinical specifics and practical context you need.
What are the diagnostic criteria for ADHD combined presentation?
ADHD combined presentation diagnosis in adults requires meeting the 5+ symptom threshold in both the inattention cluster and the hyperactivity-impulsivity cluster simultaneously. This is a symptom-count driven diagnosis, not a judgment call. Every criterion must be satisfied before a clinician can assign this presentation.
The formal criteria, as outlined by the American Academy of Family Physicians (AAFP) for adults aged 17 and older, include the following:
- Five or more inattentive symptoms present for at least six months, at a level that is inconsistent with developmental level and causes direct negative impact on daily functioning.
- Five or more hyperactive-impulsive symptoms present for the same duration and causing the same level of impairment.
- Onset before age 12. Symptoms must have been present, even if undiagnosed, before the age of 12.
- Symptoms present in two or more settings. This means impairment is documented at work, at home, in relationships, or in academic settings. Symptoms limited to one environment do not meet criteria.
- Clear evidence of impairment. Symptoms must interfere with or reduce the quality of social, academic, or occupational functioning.
Note that children require six or more symptoms per cluster, while adults need only five. This distinction matters because hyperactivity often becomes less overt with age, and the lower threshold reflects how symptoms present differently in adult life.
Clinicians use structured self-report and collateral history from multiple life domains to accurately classify ADHD presentation in adults. This means your provider may ask a partner, family member, or close colleague to contribute observations. A diagnosis based only on a single questionnaire or one clinical visit is incomplete.
Pro Tip: Before your evaluation, write down specific examples of how symptoms show up at work and at home separately. Concrete, setting-specific examples help your clinician confirm the multi-setting requirement and reduce the risk of misclassification.
How do ADHD combined type symptoms affect daily life?
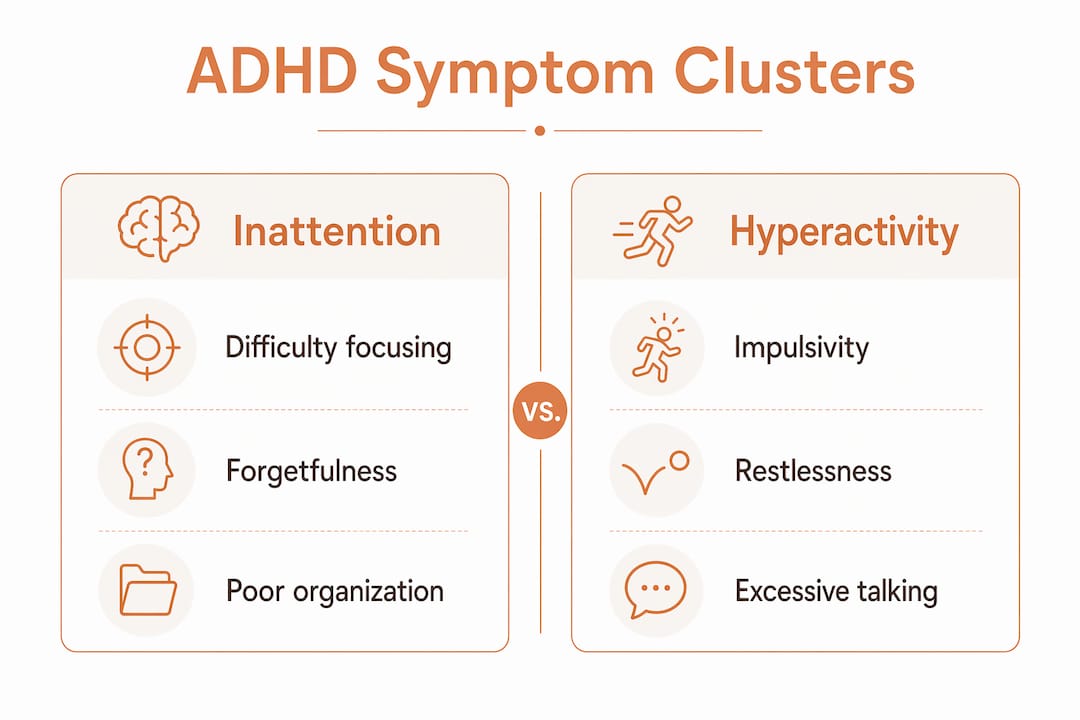
ADHD combined type symptoms are not simply “being distracted and hyper.” They appear as two distinct but overlapping behavioral patterns that can shift in intensity depending on the demands of your environment.
The inattentive symptoms adults most commonly report include:
- Losing focus during meetings or conversations, even when the topic matters to them
- Forgetting appointments, deadlines, or where they placed everyday objects
- Starting multiple tasks but rarely finishing them before moving to the next
- Avoiding tasks that require sustained mental effort, such as completing reports or reading contracts
- Making careless errors in work that does not reflect their actual ability
The hyperactive-impulsive symptoms look different in adults than in children. Overt physical restlessness often gives way to internal agitation. Common signs include:
- Feeling mentally “on edge” or unable to relax, even in calm settings
- Interrupting conversations or finishing other people’s sentences
- Making impulsive financial or personal decisions without fully thinking them through
- Difficulty waiting in lines, sitting through long meetings, or tolerating delays
- Talking excessively or shifting topics rapidly in conversation
What makes combined presentation particularly complex is the way these two clusters interact. As the Cleveland Clinic describes, a person with combined type ADHD might impulsively rush through a work assignment, then struggle to focus long enough to check it for errors. The result is work that is both hasty and incomplete. This pattern is not laziness or poor character. It is a neurological reality.
“The combination of inattentive and hyperactive-impulsive symptoms means that neither cluster operates in isolation. Each amplifies the challenges of the other, making daily functioning more demanding than either presentation alone.”
Symptoms also vary by setting. You might manage relatively well in a structured, low-distraction environment at home, then feel overwhelmed in an open-plan office. This variability is one reason symptoms across settings are a core diagnostic requirement, not just a clinical formality.
How does combined presentation differ from other ADHD types?
Understanding ADHD subtypes explained clearly requires knowing what each presentation includes and excludes. The three presentations share the same underlying condition but differ in which symptom clusters are clinically significant.
| Feature | Predominantly inattentive | Predominantly hyperactive-impulsive | Combined presentation |
|---|---|---|---|
| Inattentive symptoms (5+) | Yes | No | Yes |
| Hyperactive-impulsive symptoms (5+) | No | Yes | Yes |
| Most common in adults | Yes | Less common | Very common |
| Visible behavioral signs | Often subtle | More noticeable | Both present |
| Risk of underdiagnosis | High | Moderate | Moderate |
The predominantly inattentive type, sometimes still informally called “ADD,” is often missed in adults because it lacks the visible behavioral signs that prompt clinical attention. The predominantly hyperactive-impulsive type is less common in adults because hyperactivity often decreases as people age, while inattentive symptoms tend to persist or increase. Combined presentation requires meeting the full threshold in both clusters, which is why it carries a heavier functional burden than either type alone.
Presentations are also not fixed over a lifetime. An adult with a combined presentation diagnosis today may have had a predominantly hyperactive-impulsive presentation as a child. The shift in presentation reflects how the brain matures and how environmental demands change, not a change in the underlying condition. This is clinically significant because a childhood diagnosis of one type does not rule out a different presentation in adulthood.
For a closer look at how the inattentive type specifically presents, the inattentive type explained resource from Journeymhw offers a useful comparison.
Pro Tip: If you were diagnosed with ADHD as a child but your symptoms feel different now, ask your provider to reassess your current presentation. Adult presentations frequently differ from childhood diagnoses, and treatment should match your current symptom profile.
What are effective treatment options for ADHD combined presentation?
Multimodal treatment combining medication with behavioral therapies and lifestyle strategies produces the best outcomes for adults with combined presentation. No single intervention addresses both symptom clusters with equal effectiveness, which is why personalized, layered care is the standard of practice.
Medication options are typically the first line of clinical intervention:
- Stimulant medications such as amphetamine salts (Adderall) and methylphenidate (Ritalin, Concerta) are the most studied and widely prescribed options for combined presentation. They work by increasing dopamine and norepinephrine availability in the prefrontal cortex.
- Non-stimulant medications such as atomoxetine (Strattera) and viloxazine (Qelbree) are prescribed when stimulants are contraindicated, cause intolerable side effects, or when co-occurring anxiety is present. These take longer to show effect but are a clinically valid alternative.
- Medication dosing requires regular reassessment. What works at one life stage may need adjustment as demands and biology change.
Behavioral and psychological therapies address the skill deficits that medication alone does not resolve:
- Cognitive-behavioral therapy (CBT) adapted for ADHD targets the thinking patterns that drive impulsive decisions and avoidance behaviors. Therapists like those trained in the Safren CBT-ADHD protocol specifically address adult symptom patterns.
- Skills-based coaching focuses on time management, task initiation, and prioritization. This is distinct from therapy and complements it.
- Dialectical behavior therapy (DBT) skills training is increasingly used for adults with combined presentation who struggle with emotional dysregulation alongside core ADHD symptoms.
Lifestyle and organizational strategies are not optional add-ons. They are active components of a treatment plan:
- Time-blocking and external structure tools such as Google Calendar, Todoist, or physical planners reduce the cognitive load of self-managing attention.
- Regular aerobic exercise, specifically 30 or more minutes of moderate-intensity activity, has documented effects on dopamine regulation and executive function.
- Sleep hygiene is critical. ADHD and sleep disruption are closely linked, and poor sleep amplifies both inattentive and hyperactive-impulsive symptoms.
- Reducing environmental distractions through workspace design, noise-canceling headphones, or structured routines creates conditions where your brain can function more effectively.
For a detailed breakdown of lifestyle-based approaches, the ADHD lifestyle treatment guide from Journeymhw covers practical strategies organized by symptom type. Understanding why ADHD treatment improves daily function can also help you set realistic expectations before starting care.
Key takeaways
ADHD combined presentation is diagnosed only when an adult meets the full five-symptom threshold in both the inattentive and hyperactive-impulsive clusters, with impairment confirmed across multiple settings.
| Point | Details |
|---|---|
| Dual symptom threshold required | Adults need 5+ symptoms in both clusters, not just some symptoms in each area. |
| Multi-setting impairment is mandatory | Symptoms must cause impairment at work, home, or in relationships, not just one environment. |
| Presentations shift over time | A childhood diagnosis may not match your adult presentation; reassessment is clinically appropriate. |
| Multimodal treatment is standard | Medication plus CBT and lifestyle strategies outperforms any single intervention for combined type. |
| Misclassification risk is real | Incomplete history from only one setting is the most common cause of incorrect presentation labeling. |
What I’ve learned from watching combined presentation get missed
From my perspective, the most underappreciated clinical reality of ADHD combined presentation is how often it gets misread as two separate problems. Adults come in having been told they have anxiety, or depression, or a personality issue, when what they actually have is a neurological condition that produces both restlessness and inattention at the same time. The overlap with anxiety symptoms is particularly common and genuinely confusing, even for experienced clinicians.
What I have also observed is that adults with combined presentation often develop sophisticated coping strategies that mask their symptoms in clinical settings. They appear organized, articulate, and self-aware during an evaluation, then return home to a life that feels completely unmanageable. This is why collateral history across domains is not just a procedural checkbox. It is the difference between an accurate diagnosis and a missed one.
The other thing worth saying directly: combined presentation is not a more severe version of ADHD that you should feel worse about having. It is simply a more complete picture of how your brain works. The adults I have seen make the most progress are the ones who stop trying to manage symptoms through willpower alone and commit to a structured, multimodal plan. That shift in approach changes everything.
— Jamie
Get evaluated and treated for ADHD with Journeymhw
If what you have read here sounds familiar, the next step is a structured evaluation with a provider who understands adult ADHD presentations.
Journeymhw offers virtual psychiatric evaluations and personalized medication management for adults in Texas and Colorado, with quick appointment availability and no lengthy waitlists. Whether you are seeking an initial diagnosis or want to reassess a previous one, the process is designed to be clear and accessible from your home. Adults in Texas can access specialized ADHD care in Texas, while those in Colorado can explore ADHD treatment in Colorado through Journeymhw’s telehealth platform. You do not have to keep managing symptoms without a clear plan.
FAQ
What is ADHD combined presentation in simple terms?
ADHD combined presentation means you meet the clinical criteria for both inattentive and hyperactive-impulsive symptoms at the same time. The CDC defines it as having significant symptoms from both clusters, not just one.
How many symptoms are needed for a combined presentation diagnosis in adults?
Adults aged 17 and older need at least five symptoms from the inattention cluster and five from the hyperactivity-impulsivity cluster, both persisting for six or more months. The AAFP adult criteria also require that symptoms appear in two or more settings and began before age 12.
Can your ADHD presentation change from childhood to adulthood?
Yes. ADHD presentations are not fixed, and adults frequently have a different presentation than they did as children. The Cleveland Clinic notes that hyperactivity often decreases with age while inattentive symptoms may persist or become more prominent, which can shift a person’s clinical classification.
Is combined presentation harder to treat than other ADHD types?
Combined presentation requires addressing two symptom clusters rather than one, which means treatment plans typically need to be more layered. Multimodal care combining stimulant or non-stimulant medication with CBT and structured lifestyle strategies produces the strongest outcomes for this presentation.
How is ADHD combined presentation different from anxiety?
Both conditions can produce restlessness, difficulty concentrating, and sleep problems, which is why they are frequently confused. The key distinction is that ADHD symptoms are present across multiple settings and began in childhood, while anxiety symptoms are often tied to specific triggers or situations. A thorough evaluation that includes history from multiple life domains is the most reliable way to differentiate them.